Mosaicism in Angelman Syndrome
By Dr. Charles A. Williams, Professor of Pediatrics and Genetics, Division of Genetics and Metabolism, Department of Pediatrics, University of Florida, Gainesville, FL
In the last edition, I reviewed the four genetic mechanisms that can disrupt the Angelman syndrome (AS) gene: chromosome deletion, imprinting defect, mutation in UBE3A and paternal uniparental disomy. When an individual with AS has one of these defects, it is typically present in every cell of the body, since the defect existed at the time of conception when the sperm and egg fused to form the first cell of the embryo. All of the subsequent cells are thus derived from this original cell. It is possible in rare situations however for the AS defect to occur after the first cell divisions of the embryo such that there is a normal and an abnormal cell line; the general term for this phenomenon is cell mosaicism.
 Mosaicism in an individual with AS means that a few cells in their body (and also in their brain) are normal. These normal cells coexist with all of the other cells that have the AS defect. Mosaicism in AS most often occurs in imprinting defects that do not involve deletions of the imprinting center (the great majority of those with imprinting defects are of this non-deletion type). About 10 to 30% of individuals with the non-deletion type may have a small percent of their cells that are normal.
Mosaicism in an individual with AS means that a few cells in their body (and also in their brain) are normal. These normal cells coexist with all of the other cells that have the AS defect. Mosaicism in AS most often occurs in imprinting defects that do not involve deletions of the imprinting center (the great majority of those with imprinting defects are of this non-deletion type). About 10 to 30% of individuals with the non-deletion type may have a small percent of their cells that are normal.
We detect evidence of this by the DNA methylation test that is performed on blood. When the test suggests mosaicism, we presume (but do not really know) that cells in the brain also have a similar percentage of normal cells. In instances of imprinting mosaicism, the percent of normal cells is usually less than 20%. Individuals with AS who are imprinting-type mosaics can have relatively higher developmental ability. Some have been noted to speak words and even to put words together, more than is seen in the typical child with AS who is non-mosaic. They may also have better motor ability (e.g., almost normal walking) and relatively higher cognitive skills The three other mechanisms that cause AS are much less likely to have mosaicism but a few rare instances have been reported. Chromosome studies (either molecular or FISH-type) may identify a small percent of cells without the typical 15q11.2-q13 deletion. For example, 80% of the cells in the blood may have the typical AS deletion while 20% of the cells are normal. The same can theoretically occur for those with AS due to uniparental disomy. To my knowledge, mosaicism for UBE3A mutation, identified by blood study in an individual with AS, has not been reported but that is also theoretically possible.
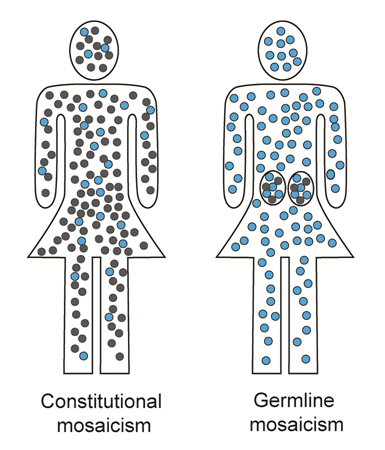
In a mother who has an AS child with a UBE3A mutation, mosaicism involving UBE3A has been detected in her in what is termed “germline” mosaicism. Here, the mother’s blood cells are normal but apparently in her ovaries there are egg (e.g., germ) cells that have the UBE3A mutation. This situation is presumed to be present, for example, when the mother gives birth to two subsequent children with AS, each having the same UBE3A mutation, but studies of the mother’s blood are completely normal. The diagram illustrates this type of germline mosaicism (blue cells are the normal cells) and contrasts it to the other type of mosaicism that is discussed above, termed “constitutional” meaning that cells throughout the body are involved.
Understanding mosaicism in AS can be complicated especially when considering the possibility of germline mosaicism in mothers, since this rare condition can lead to recurrence of AS among siblings.